
Wellbeing: Death by Flour
The hidden dangers of sugar, refined carbs, folic acid, preservatives, pesticides, and potassium bromate

Our European travels have given us a glimpse of how people on the other side of the pond eat. One noticeable difference is what is consumed at breakfast. Those vast European buffets at the various restaurants provide a window into the eating habits of those who frequent them. Generally, commercial cereals are not offered, although granola (in a big bowl) usually is. Plain, unsweetened yogurt is a go-to for most, eaten with fruit and sometimes topped with nuts. Milk is available, but not prominent, and is rarely used for the granola. Meats, eggs, and cheese are prominently displayed and eaten. Tomatoes, mushrooms, beans, and such like are often available - either cooked or raw. Fresh bread—baked locally — is offered, but it is much less prominently displayed or consumed. It is always on the counter as a loaf, and one is supposed to cut off a piece with a large, serrated knife. With a half slice being the usual serving size. Yes, there are usually some sweet breads- croissants and such like, but again, they aren’t the main “go to” for most people.
So, basically, the emphasis is on protein, fermented dairy, and produce. With grain products being less prominently displayed or eaten. The eating patterns are noticeably different. The other thing is that people take less onto their plates and tend to clean their plates. People just seem to eat cleaner.
Clean eating is a dietary approach that focuses on consuming whole foods and foods in their most natural, unprocessed states. Jill and I do not have perfect eating habits, but our diet has undergone a radical change, and the results have been phenomenal. One of the most critical steps on our road to a different way of eating was eliminating all breakfast cereals from our diet a few years ago.
Breakfast cereal and sugar
Breakfast cereals are evil. Not just for us, but for all Americans: children and adults alike. If this wasn’t bad enough, Americans have been spoon-feeding this junk to toddlers as soon as a spoon could fit in their tiny mouths. Cereal is now eaten as breakfast, an afternoon snack, for dinner, and as dessert. Cereal is promoted as a healthy food, yet… it isn’t. Breakfast cereals are made up primarily of the basic forms of carbohydrates: starches and sugars.

On average, children’s cereals are made up of 34 percent sugar by weight, and most children in the USA eat about ten pounds of sugar each year from cereal alone. Furthermore, some children consume large amounts of cereal, far exceeding the relatively small serving size listed on the box. Some of the cereal brands contain over 50% sugar by weight – they are essentially pure sugar and simple carbohydrates!
Much of the sugar in those cereal boxes comes from high-fructose corn syrup, which is highly addictive. High fructose corn syrup is considered an ultra-processed food. The manufacturing process utilizes enzymes and acids to convert some of the glucose from corn syrup into fructose, a sweeter-tasting compound. You may ask why high-fructose corn syrup is used. This sweetness makes the stuff even more addictive, especially for little kids.
Human Kibble

That said, sugary cereals are also addictive. Many people eat multiple bowls of cereal daily. Many children eat multiple bowls of cereal a day. Let’s face it, cereal is easy, cheap to buy, safe to prepare, palatable and readily available. Even a six-year-old can pull out a box of cereal, get a bowl, pour milk on top, and generally not get hurt doing so. But it isn’t just the cereal that people eat; they also top the cereal bowl with sugar. That means lots of excess calories. Cereal contributes to obesity, as it is a low-quality, high-carb food, and because it is addictive, it adds excess calories to one’s daily diet
Mikey Likes It! Life cereal advert.
Then there are the preservatives and additives commonly found in most commercial cereal brands. BHT and BHA are two of the preservatives commonly found in commercial cereals, bread, and snack foods sold in the United States.
Preservatives
BHT (Butylated Hydroxytoluene) is used to extend shelf life, especially in cereals such as Cap’n Crunch, Apple Jacks, and Froot Loops. It is classified as a possible human carcinogen by the International Agency for Research on Cancer (IARC) and has been associated with hormone disruption and potential reproductive harm. BHT is incorporated either directly into the cereal or through packaging liners, which can transfer it into the food.
BHA (Butylated Hydroxyanisole) is a chemical similar to BHT, sometimes present in cereals, though it is more often used for preserving meats. It is classified as possibly carcinogenic and has been linked to hormone disruption.
Artificial food dyes
Artificial food dyes, such as Red 40, Yellow 5, Yellow 6, and Blue 1, are commonly used in breakfast cereals and snack foods to enhance their visual appeal, particularly for children. Some dyes, such as Red 40 and Yellow 5, are banned in children’s foods in the European Union due to links to hyperactivity and other health concerns, but remain legal in the United States. Under President Trump, the use of these dyes is being restricted; however, the ban on these dyes will not take effect until the end of 2026.
Folic acid
Folic acid is added to breakfast cereals, flour, and grain as a substitute for natural folate acid. This is added so that pregnant women make adequate amounts of folate to prevent neural tube defects (Spina bifida and Anencephaly) in babies and to help meet the minimum folate standards. Of note, the U.S. FDA has mandated the enrichment of wheat flour, cornmeal, and rice flour with folic acid (140 µg per 100 g of flour) since 1998.
For breakfast cereal fortification, a folic acid solution or powder is sprayed or mixed onto the finished cereal before packaging. It is also required for meal replacement (protein) bars and powders. Of course, it isn’t just breakfast cereals; folic acid is in all of our bread - unless it is made with organic flour.
Most people tolerate this supplement well. However, roughly 30–40% of the population carries a genetic mutation called MTHFR polymorphism, which reduces their ability to metabolize folic acid efficiently. And for 10-15% of the population, their bodies do not properly break down folic acid, leading to unmetabolized folic acid (UMFA) buildup in the blood, which may weaken immune function, including natural killer (NK) cell activity.
There can also be significant methylation-related issues in those with MTHFR polymorphisms, leading to elevated homocysteine levels despite adequate folic acid intake.
High homocysteine levels mainly increase the risk of cardiovascular and neurological disease. Chronically elevated levels can damage blood vessel linings, promote arterial plaque buildup and blood clots, and are linked to higher rates of heart attack and stroke. In the brain, excess homocysteine contributes to oxidative stress and impaired neurotransmitter function, raising the risk of cognitive decline, dementia, depression, and neuropathy, especially when folate or vitamin B12 is low.
In pregnancy, high homocysteine is associated with miscarriage, preeclampsia, and birth defects such as neural tube defects. Overall, it’s a marker of impaired methylation and B-vitamin deficiency, with vascular and neurological damage being the most common and clinically significant consequences.
There is a simple blood test widely available to analyze for MTHFR variants. The test looks for two main DNA variants (SNPs) in the MTHFR gene:
C677T (rs1801133) is the MTHFR gene most strongly linked to reduced enzyme activity and,
The A1298C (rs1801131) gene, which has milder effect, but can compound with C677T
The results of a lab report testing for the variants will report on whether an individual has the following profile:
Normal (wild type)
Heterozygous (one copy of the variant)
Homozygous (two copies, most substantial effect)
Because of the higher risk of cardiovascular disease associated with the MTHFR gene and the lack of overt symptoms, we recommend that everyone consider getting tested. However, some groups of people are more likely than others to have one of these variants.
The geographic and Ethnic Distribution of the Frequency of C677T Allele differs:
East Asian (China, Japan, Korea) - 30–40% homozygous - Among the highest prevalence globally; linked to high homocysteine levels and folate sensitivity.
Southern European (Italy, Spain, France, etc.) - 10–20% homozygous - Moderate frequency; often associated with mild enzyme reduction.
Northern European - 5–12% homozygous - Common but less than in Mediterranean regions.
African and African American - <2–3% homozygous -The 677T variant is rare; A1298C is somewhat more common.
Indigenous American (including S. Americans) - Variable (10–30%) - Reflects East Asian ancestry patterns.
South Asian (India, Pakistan)- 10–15% homozygous.
Older studies and meta-analysis studies have not been conclusive regarding the association between the C677T gene and cardiovascular disease, but more recent studies have found that, especially in Asian populations, the risk is higher:
“We observed a significant correlation between the MTHFR C677T polymorphism and the development of CHD in the recessive model (OR: 1.35, 95% CI: 1.06-1.71, P = 0.006) for the overall population.
In subgroups stratified by ethnicity and source of controls, subgroup analyses indicated similar associations in Asians and hospital-based groups, but not for Caucasians and population-based groups.” (ref).
Our findings indicated that MTRR rs1532268, MTHFR rs1801131 and MTHFR rs1801133 polymorphisms may affect the risk of CHD in Asians and Caucasians, while the MTRR rs1801394 polymorphism may only affect in risk of CHD in Asians (ref).
And yet still, no major medical group or the HHS “task force” recommends testing, not even for the Asian population, who are most at risk. Particularly if eating a high-carb (cereal/bread/etc) diet - as the amount of folic acid being ingested could be quite high in those individuals.
The real reason why folic acid supplementation is required is to prevent neural tube defects, and those numbers have decreased by 36% since folic acid was added to foods so that pregnant women can get adequate amounts. Neural tube defects have declined from around 4,100 cases per year to around 3,000 - so this truly has been a blessing for some families. This is important, but the only people being affected by this mandated supplement are pregnant women and their babies. Are the neural tube defect benefits sufficient to justify the harms done to those with MTHFR gene C677T genetic alleles? No one has done the risk/benefit analysis to the best of my knowledge. So I asked Grok to perform the analysis (see below at the end of this essay).
Potential Harms of Folic Acid supplementation are primarily associated with excessive intake (>1,000 mcg/day). At high doses, unmetabolized folic acid (UMFA) can accumulate, especially in TT carriers due to impaired conversion, potentially creating a “pseudo-MTHFR deficiency” by further suppressing enzyme activity.
Evidence for harm is mostly associative (from observational studies and meta-analyses), not causal, and focused on excess rather than standard use. No large randomized trials show definitive risks at 400 mcg.
Once again, this is a public mandate to supplement all grains for which we, the public, weren’t given a choice. And the results are that for some, the risk of cardiac heart disease, immune dysfunction, and cognitive issues may be significant. Another example of “Public Health” officials mandating a one-size-fits-all solution based on flawed utilitarian (greatest good for the greatest number) logic.
BTW- the CDC does not address the issues directly, but instead focuses on the need for folic acid supplements for pregnant women, yet there are alternatives such as methylated folate, which is a natural form of folate and more like one would eat in whole foods. The problem is that 5-MTHF (methylated folate) and folinic acid most likely will improve folate status - but until clinical trials demonstrating fewer NTDs have been conducted, the CDC will not recommend them. As the CDC finds folic acid adequate, there is little incentive for the government to fund such studies. So, guidelines continue to recommend folic acid specifically. But there are many “methylated folate” supplements on the market.
Of course, the real solution may be a whole-foods diet that avoids refined carbohydrates and concentrates on nutrient-dense foods. Here is a list of foods generated from an AI - that contain high amounts of folate:

Because of FDA regulations (7 CFR §205), products labeled “organic” or “100% organic” cannot include synthetic nutrients like folic acid, unless specifically approved on the “National List of allowed substances”, and folic acid is not on that list. So, buying organic flour, rice, and rolled oats, for instance, is a good way to avoid folic acid supplementation if one tests positive or if one’s status is unknown for the MTHFR gene.
Various calculations suggest that supplementation levels are not high enough to warrant concern for heterozygotes of the MTHFR gene. Although, frankly, for those who eat many servings a day of breakfast cereals, bread, or other grains, the actual effect of the continuous and probably over ingestion of folic acid is unknown. But for homozygous individuals, folic acid supplementation is a real issue, particularly if one’s diet includes commercial (non-organic) grain products, such as bread and cereal.
If one can’t metabolize excess folic acid in the body, then low methylation occurs. Low methylation is linked to a sluggish metabolism, generally high inflammatory blood enzyme markers (chronic inflammation), and poor DNA repair. Meanwhile, balanced methylation promotes healthy gene expression, a resilient mood, efficient detoxification, and stable hormones. Therefore, those with two copies of the MTHFR gene are at much higher risk of cardiovascular disease and should take this very seriously.
So why is it that people who have higher frequencies of these genes or of Asian heritage are not warned about the dangers of ingesting too much folic acid?
Pesticide contaminants
Cereal grains are also a significant source of pesticide contaminants, including glyphosate, which is linked to a whole cornucopia of diseases, as discussed in other Malone News articles:
Weed Killer and Autism (ASD) or ADHD?
Dr. Robert W. Malone. April 19, 2023
We all know that glyphosate and other herbicides are sprayed on almost all of our commercial grains, legumes and seed oil crops to kill the plants all at once, thus making the processing much easier. These desiccants, as they are called, are found in trace amounts in our commercial grains and seed oils as well as legumes. That means in our breads, flou…
Atrazine and the "Bent Science"
Dr. Robert W. Malone. June 20, 2023
It is not the job of the USDA or the EPA to feed the world or control climate change. It is the job of these Federal agencies to protect the food supply and the environment for the peoples of the United States.
Well being: The Glyphosate Addiction
Dr. Robert W. Malone. September 21, 2024
We are up in the sky, flying home from San Antonio early on this Saturday morning. Once home, we have a full day’s work. I am re-recording the introduction of the new “PsyWar” book - as that particular section was the first recorded and ended up with a few little glitches. Jill will unpack, do laundry, and prepare to leave for Tokyo on Monday morning…
Potassium bromate
Then there is potassium bromate in bread, which some commercial bakeries use to produce bread with a higher rise and firmer texture. It helps the dough hold gas during proofing and creates a uniform crumb and white color. Perfect for mass production!

Potassium bromate is classified as a possible human carcinogen (Group 2B) by the International Agency for Research on Cancer (IARC). Animal studies have linked it to kidney and thyroid tumors. The concern is that bromate residues can remain in finished bread if baking temperatures or times are inadequate to convert it to non-toxic bromide fully.
Potassium bromate addition to food is banned or restricted in the EU, UK, Canada, Brazil, China, Japan, and many other countries, but is still allowed to be used in the USA. So, this is another ingredient to check out when reading food labels. Specifically look for “potassium bromate” or “bromated flour.
Wrapping it up
All of these additives have raised health concerns, particularly when compared to regulations in other countries. As market sales of cereal in the USA for 2024 topped over 13 billion USD and make up a significant percentage of the calories eaten by Americans each day, it is easy to see how breakfast cereals have contributed to the rise in obesity, a decline in healthy immune function, and a risk of cardiovascular disease.
There are many ideas about why obesity and being overweight are so prevalent in the USA. According to one model, the quality of food consumed, particularly the intake of processed carbohydrates, plays a critical role in body weight management rather than just total calorie intake. This theory posits that the key to avoiding obesity is to forego processed carbohydrates and instead focus on whole foods, which are effective tools for weight loss and maintenance. This is precisely what Jill and I do. It is not just the quantity of food intake that affects obesity, but also its quality.
Many studies have documented that commercially grown grain cereals, as well as produce, lack many micronutrients because the soil these grains are grown in has been depleted of them. So, people consume vast amounts of breakfast cereals, but, aside from the usual fortifications found in most boxed cereals, they lack many micronutrients and minerals. So, the body craves more and more calories and yet never gets enough adequate nutrition. The end result is that adults and children alike pack on the pounds.
Some of the tricks that we do to avoid commercial grain products are to cook your own. We bake most of our own bread with organic flour, avoid all boxed breakfast cereals, and stick to an occasional breakfast of porridge made with organic oats and whole milk. We consider this a fundamental part of homesteading - the art and science of living in our home rather than outside it.
This is why we all need to get back to traditional, whole foods and stay away from flour, and basically all refined carbohydrates – just like our ancestors ate. Cause those carbs are killing us with satiation.
The opinions expressed in this essay are my own, and do not claim to represent the opinions of the US Government (USG), the Centers for Disease Control and Prevention (CDC), or the Advisory Committee on Immunization Practices (ACIP).
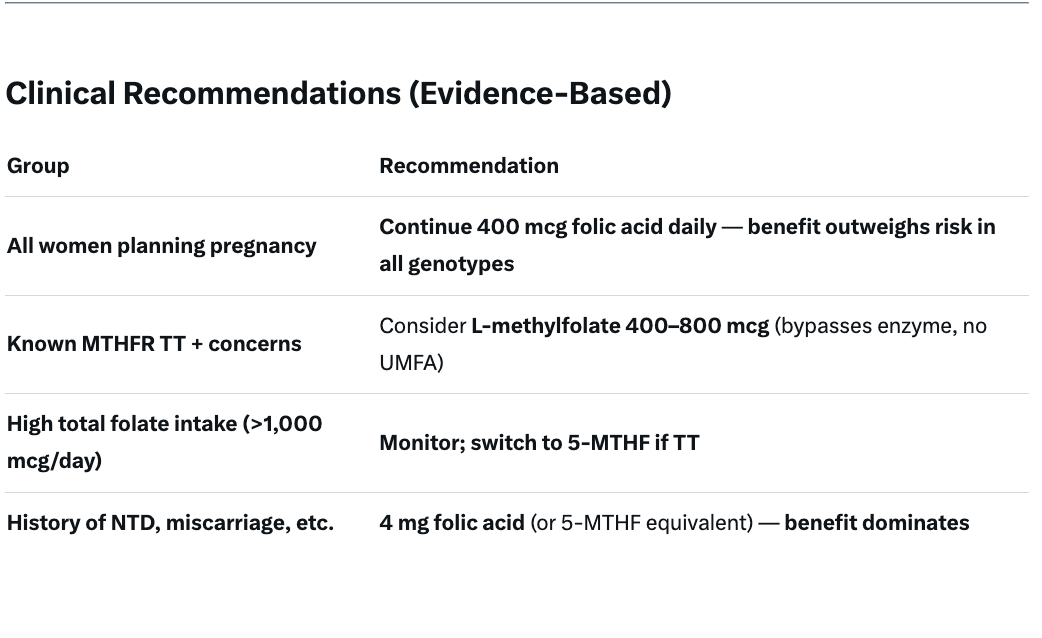
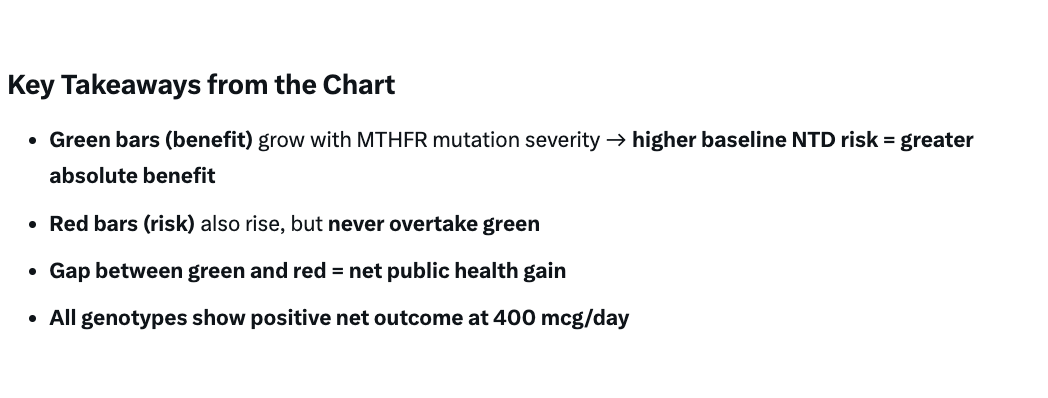
Folic Acid Risk Benefit Analysis for Individuals with MTHFR C677T alleles
Grok-generated quantitative risk-benefit analysis of folic acid supplementation (400 mcg/day) specifically for individuals with MTHFR C677T alleles (CT or TT genotypes), based on the best available meta-analyses, cohort studies, and clinical guidelines as of 2025.
This is an example of how risk-based public health analyses need to be performed.
NTDs = Neural Tube Defects
(Note that this risk/benefit analysis was done for pregnant women only, and excluded non-pregnant people from the analysis).












When I asked the followed Grok to do the analysis for non-pregnant people ingesting 1000 mcg per day, the summary answer was as follows;
Quantitative Risk-Benefit Analysis of Folic Acid Supplementation (100 mcg/day) for Non-Pregnant Individuals with MTHFR C677T (CT or TT Genotypes)
Quantitative Risk-Benefit Analysis of Folic Acid Supplementation (1000 mcg/day) for Non-Pregnant Individuals with MTHFR C677T (CT or TT Genotypes)OverviewA 1000 mcg/day dose is 2.5× the standard 400 mcg recommendation and falls in the “high-dose” category in most meta-analyses (>800–1000 mcg). It effectively normalizes folate status and lowers tHcy across MTHFR genotypes, with greater absolute benefit in TT due to higher baseline tHcy (~2–4 µmol/L higher than CC).
However, risks emerge at this dose, particularly in individuals with pre-existing conditions (CVD, cancer history, B12 deficiency). Key 2025 Guidelines (CDC, USPSTF, WHO):
Do not recommend >400 mcg/day routinely in non-pregnant adults.
No genotype-specific dosing for MTHFR C677T.
Upper tolerable limit (UL) = 1000 mcg/day from supplements/synthetic sources (IOM 1998; unchanged 2025).
Unmetabolized folic acid (UMFA) appears in plasma at >800 mcg/day and is dose-dependent; TT individuals clear UMFA more slowly (~20–30% higher UMFA AUC).
Evidence from dose-stratified meta-analyses (2020–2025) and MTHFR-genotyped cohorts shows diminishing returns beyond 400–600 mcg and emerging harm signals at 1000 mcg, especially in TT homozygotes
